- polycystic ovarian syndrome (PCOS)
- androgen-producing adrenal and ovarian tumours
- congenital adrenal hyperplasia (CAH)
- Cushing's syndrome.
Congenital adrenal hyperplasia (CAH)
 |
| Fig 1: Congenital Adrenal Hyperplasia |
 |
| Fig 2: Congenital Adrenal Hyperplasia Female |
 |
| Fig 3: In the adrenal gland, cholesterol is turned into a precursor called pregnenolone, then several enzymes complete the production of aldosterone, cortisol and androgens. A deficiency in the enzyme 21-hydroxylase leads to inadequate amounts of aldosterone and cortisol (green); other substances that do not need the defective enzyme are produced in excess (blue). This enzyme deficiency is inherited and is the most common cause of congenital adrenal hyperplasia (CAH). |
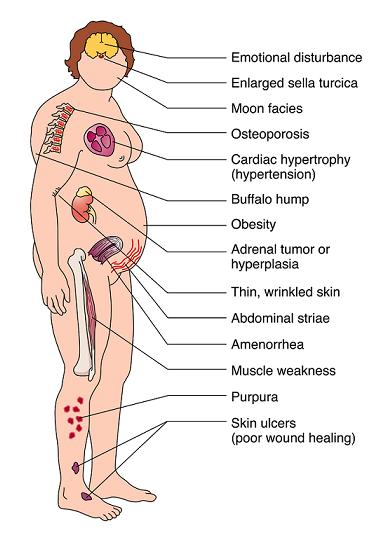
Cushing's Syndrome
 |
| Fig 4: Signs of Cushing's Syndrome |
Menstrual irregularities, hirsutism with virilisation and weight gain are features that may be present in Cushing's syndrome, hence estimation of 24 hours urinary free cortisol on at least two occasions is a good screening test.
Estimation of serum testosterone, other androgens, sex hormone binding globulin (SHBG) and free androgen index (FAI), will be important in all of the above conditions as hyperandrogenism may be present in all of them.
Imaging of adrenals and ovaries, such as CT or MRI scans, is relevant in the above setting but obviously there will be some further indications on basic examination and investigations to suggest the possibility of adrenal tumour, hyperplasia or ovarian tumour.
Estimation of gonadotrophins (follicle-stimulating hormone (FSH) and luteinizing hormone (LH)) along with androgens and estrogen, is important in the given presentation but there is no indication to perform a gonadotrphin-releasing hormone test. This test is done as a part of the combined triple test in suspected hypopituitarism and in the investigation of delayed puberty.
Fig 1, Fig 2, Fig 3, Fig 4,
{kind=link}
{kind=link}
{kind=link}
{kind=link}
No comments:
Post a Comment